

Megaloblastic anemia is a type of anemia characterized by the presence of abnormally large, immature red blood cells (megaloblasts) in the bone marrow and peripheral blood. This condition primarily results from deficiencies in vitamin B12 (cobalamin) and/or folic acid (vitamin B9). These vitamins are crucial for DNA synthesis and red blood cell production. This note explores the causes, pathophysiology, symptoms, diagnosis, treatment, and prevention of megaloblastic anemia due to vitamin B12 and folic acid deficiencies.
Causes of Megaloblastic Anemia
Vitamin B12 Deficiency
1. Dietary Insufficiency: Inadequate intake of vitamin B12, commonly seen in strict vegetarians or vegans since B12 is primarily found in animal products.
2. Malabsorption Syndromes:
Pernicious anemia: An autoimmune condition where intrinsic factor (necessary for B12 absorption) is deficient. Gastrointestinal surgeries (e.g., gastrectomy, ileal resection) that remove parts of the stomach or small intestine. Conditions like Crohn’s disease or celiac disease that affect the ileum where B12 is absorbed.
3. Other Causes: Chronic use of proton pump inhibitors or H2 blockers, which reduce stomach acid necessary for B12 absorption. Parasites (e.g., fish tapeworm) or bacterial overgrowth in the intestines.
Folic Acid Deficiency
1. Dietary Insufficiency: Poor intake of folic acid-rich foods like leafy green vegetables, fruits, and fortified cereals.
2. Increased Requirements: Pregnancy, lactation, and growth spurts in infants and adolescents increase the demand for folic acid. Conditions causing rapid cell turnover, such as hemolytic anemia and malignancies.
3. Malabsorption Syndromes: Diseases affecting the small intestine, like celiac disease or tropical sprue.
4. Drug Interactions: Certain medications (e.g., methotrexate, anticonvulsants) interfere with folic acid metabolism.
5. Alcoholism: Excessive alcohol intake can impair folic acid absorption and utilization.
Pathophysiology of Megaloblastic Anemia
Both vitamin B12 and folic acid are essential for DNA synthesis. Deficiencies in these vitamins lead to impaired DNA replication and cell division, particularly affecting rapidly dividing cells like those in the bone marrow. This results in the production of large, immature, and dysfunctional red blood cells (megaloblasts) that are unable to efficiently carry oxygen. The underlying mechanisms are:
1. Vitamin B12: Acts as a cofactor for the conversion of homocysteine to methionine and the conversion of methylmalonyl-CoA to succinyl-CoA. Deficiency leads to the accumulation of homocysteine and methylmalonic acid, which disrupts DNA synthesis and causes neurological damage.
2. Folic Acid: Involved in the synthesis of thymidine, a nucleotide required for DNA replication. Deficiency impairs DNA synthesis, leading to ineffective erythropoiesis and the formation of megaloblasts.
Symptoms of Megaloblastic Anemia
The symptoms of megaloblastic anemia due to vitamin B12 and folic acid deficiencies include:
1. General Anemia Symptoms:
– Fatigue and weakness.
– Pale skin.
– Shortness of breath and dizziness.
– Heart palpitations.
2. Specific to Vitamin B12 Deficiency:
– Neurological symptoms: Numbness and tingling in the hands and feet, difficulty walking, memory loss, and cognitive impairment.
– Glossitis and mouth ulcers.
– Jaundice due to hemolysis of megaloblastic red cells.
3. Specific to Folic Acid Deficiency:
– No neurological symptoms (distinguishing feature from B12 deficiency).
– Glossitis and mouth ulcers.
– Possible hyperpigmentation of the skin.
Diagnosis of Megaloblastic Anemia
Diagnosis of megaloblastic anemia involves a combination of medical history, physical examination, and laboratory tests:
1. Medical History and Physical Examination: Assessing dietary habits, gastrointestinal symptoms, and neurological signs. Physical examination may reveal pallor, glossitis, and neurological abnormalities.
2. Laboratory Tests:
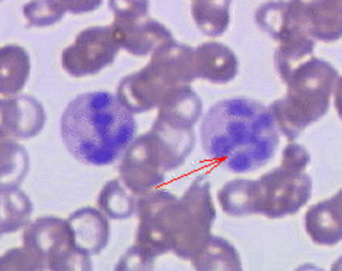
Complete Blood Count (CBC): Macrocytic anemia (increased mean corpuscular volume, MCV), hypersegmented neutrophils.
Serum Vitamin B12 and Folate Levels: Low levels confirm deficiencies.
Homocysteine and Methylmalonic Acid Levels: Elevated in B12 deficiency but not in folic acid deficiency.
Peripheral Blood Smear: Presence of megaloblasts and hypersegmented neutrophils.
Bone Marrow Examination: Hypercellular marrow with megaloblastic changes (if needed).
3. Additional Tests:
Schilling Test: Historically used to diagnose pernicious anemia (now rarely used).
Antibodies to Intrinsic Factor and Parietal Cells: For diagnosing pernicious anemia.
Treatment of Megaloblastic Anemia
Treatment of megaloblastic anemia focuses on replenishing the deficient vitamins and addressing the underlying causes:
1. Vitamin B12 Deficiency:
Dietary Modifications: Including more B12-rich foods (meat, dairy, eggs).
Oral Supplements: For those with dietary insufficiency.
Parenteral B12 (Injections): For those with malabsorption issues or severe deficiency (e.g., 1000 mcg intramuscularly weekly for 4-6 weeks, then monthly).
2. Folic Acid Deficiency:
Dietary Modifications: Including more folic acid-rich foods (leafy greens, fruits, fortified cereals).
Oral Supplements: Typically 1 mg daily.
3. Addressing Underlying Causes: Treating gastrointestinal disorders, adjusting medications, managing alcohol intake, and addressing any chronic conditions that contribute to deficiencies.
Prevention of Megaloblastic Anemia
Preventive measures for megaloblastic anemia include:
1. Balanced Diet: Consuming a varied diet rich in B12 and folic acid. For vegetarians and vegans, considering fortified foods or supplements.
2. Regular Monitoring: Especially in high-risk groups such as pregnant women, the elderly, individuals with gastrointestinal disorders, and those on medications that affect vitamin metabolism.
3. Health Education: Raising awareness about the importance of adequate vitamin B12 and folic acid intake and recognizing early symptoms of deficiency.
Conclusion
Megaloblastic anemia due to vitamin B12 and folic acid deficiencies is a significant health concern that can lead to severe complications if left untreated. Understanding the causes, pathophysiology, symptoms, diagnosis, treatment, and prevention of this condition is crucial for effective management and improving patient outcomes. Early detection, appropriate dietary modifications, and timely medical interventions can help prevent complications and ensure optimal health.